- Getting Started
- Care Coordination
- Clinical Protocols
- Care Guidelines
- Screening Tools for EDs
- Mental Health Tools for Pediatricians
- ED and Pediatrician Collaboration
- Sustaining the Work

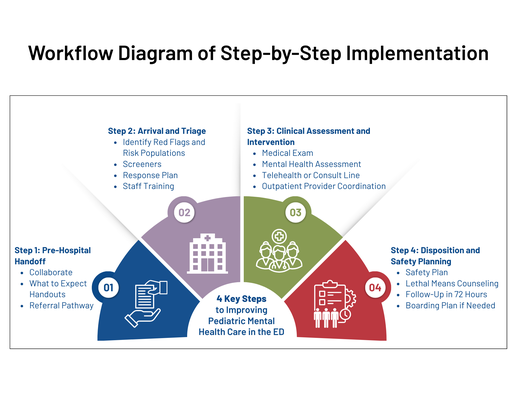
Practical guidance to support safe, coordinated, and family-centered pediatric mental health care in the emergency department. Use these steps to help guide conversations with ED providers and their staff.
Note: They are not exhaustive and should help your team better understand the current processes in place or help identify areas of opportunity to engage.
- Collaborate with EMS, pediatricians, other primary care providers, and schools to use shared screening tools and language.
- Provide a “What to Expect” handout for EMS to share with families or post on your website to help families prepare, covering topics like:
- An overview of the ED process for mental and behavioral health screening.
- What families should bring or know before arrival.
- How caregivers can provide helpful background information that supports the assessment and care.
- Develop a referral pathway that outlines:
- What information should EMS relay to the ED (e.g., presenting behaviors, recent events, known diagnoses)?
- Who to contact in the ED for additional support or clarification.
Train triage and intake staff to:
- Recognize red flags and mental/behavioral health concerns in children and adolescents.
- Identify high-risk populations (e.g., children who have experienced traumatic events, children with autism spectrum disorders [ASD]).
- Use appropriate screeners:
Ensure workflows address:
- Observation level (e.g., 1:1 monitoring)
- Environmental safety (removal of dangerous items, hospital-issued attire, avoiding utensils with food, etc.)
- Supportive triage best practices:
- Prioritize history-taking with both the child patient and the caregiver, using trauma-informed, developmentally appropriate approaches (e.g., HEADSSS).
- Work with interpreters trained in mental health terminology.
- Use developmentally appropriate and confidential screening methods.
- Support youth with ASD or sensory processing differences by moving patients to a safe, low-stimulation area.
- Reassess frequently, especially during long wait times.
- Activate escalation protocols for high-risk presentations (e.g., imminent harm, elopement risk), including security or mental/behavioral health teams as needed.
Medical screening should include:
- Physical exam and review of systems.
- Injury treatment and medical stabilization.
- Urine toxicology screen and/or pregnancy test, as needed.
Mental/behavioral health assessments should be:
- Conducted in a private space.
- Led by a pediatric-trained mental health provider or supported via telehealth.
- Comprehensive while addressing exposure to traumatic events, psychiatric history, family dynamics, substance use, and risk factors.
When in-person mental health providers aren’t available:
- Engage PMHCA consult lines for clinical guidance and planning.
- Use tools like SAFE-T or BSSA.
- Develop collaborative safety plans with families, not just forms.
- Provide lethal means counseling and distribute tools like lockboxes or safety brochures.
- Schedule follow-up care within 72 hours and confirm details with families prior to discharge.
- Maintain a list of hospitals with pediatric inpatient psychiatric services with admission criteria.
- Provide a staff checklist for transport, documentation, and family communication.
- Ensure ongoing patient safety (e.g., monitor for access to harmful items, assign 1:1 sitter if needed)
- Provide daily structure (e.g., meals, hygiene access, rest periods)
- Limit stimulation by removing personal devices if they are disruptive to the patient’s psychological well-being, but this should be done cautiously due to the high risk for escalation (and isolation from peer supports)
- Offer calming and distracting activities
- Continue regular reassessment, medication management, and safety planning efforts