Abnormal Vital Signs: Intervention Bundle

Abnormal vital signs are key in the early identification of critically ill and injured patients, and have been associated with increased ED return rates; their early identification ensures patients receive the appropriate level of care and resources needed (1). Several pediatric clinical prediction rules have included vital signs in their analysis of the likelihood of sepsis in febrile children. Each year, tens of thousands of children are treated for severe sepsis in the United States (US), resulting in substantial morbidity and mortality, and nearly $5 billion in US health care expenditures (2-3). Early recognition of abnormal vital signs is associated with improved outcomes for patients with sepsis (4-5).
Identifying abnormal vital signs in pediatric patients is challenging since heart rate, respiratory rate, and blood pressure vary with age. Furthermore, vital signs may reflect anxiety, fever, or pain rather than the clinical deterioration of the child. In addition, most children in the US present EDs in centers with low pediatric volumes and little exposure to pediatric sepsis (6), contributing to the challenge of sepsis recognition. Many different pediatric sepsis screening tools and early warning systems include the identification of abnormal vital signs coupled with bedside clinician assessment and are associated with improved recognition and decreased cases of missed sepsis (7-10).
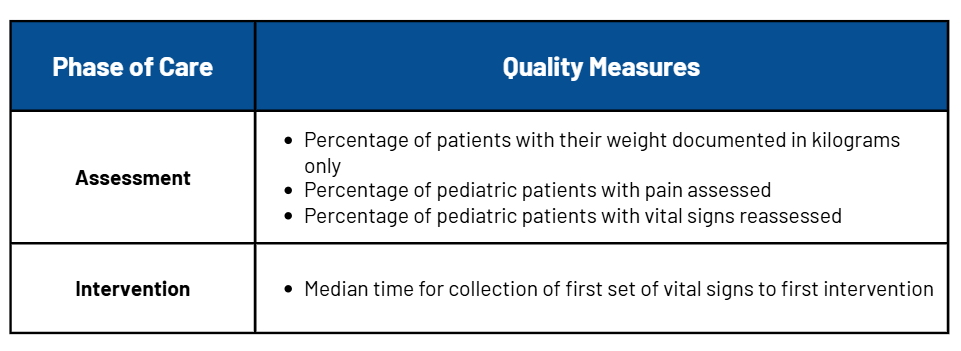
This intervention bundle is designed to help guide PRQC teams that want to implement change strategies specific to the clinical care process for children who present to the ED with abnormal vital signs. Teams can select to work on an intervention specific to abnormal vital signs for their quality improvement project. It is anticipated that individual hospital/facility teams will choose one or more measures to work on. The following measures are included within the National Pediatric Readiness Quality Initiative (NPRQI), where you will enter select data. Please see here to learn more about quality measures development.
The quality measures related to abnormal vital signs are:
Gathering data when implementing changes to your system is important. Data collection allows you to measure how your implementation is going and if your changes are moving towards your process measure goal. Data and measurement can help you give insight into how the changes are being accepted or not accepted into your system.
There are a variety of ways to assess how your implementation is going. Some include:
- Chart audits to evaluate the process measure above
- Can be conducted in real-time or retrospectively; may be automatically set up in a report to capture the pain assessment field from the flowsheet
- Can be all charts or a representative sample of charts selected for surveillance using a random or systematic sampling approach (e.g., every 5th pediatric patient over 10 years old, or all pediatric patients evaluated over a given time period).
- Survey staff on usage and/or comfort with pain scores and treating pediatric pain
- Consider surveying staff experience and satisfaction with the implementation to better learn from your intervention strategies
- Create a brief survey for families for any of the process measures above
Some example numerical metrics you can calculate for each process measure are in the table Abnormal Vital Signs Process Measure
Below you will find suggested possible interventions, also called change strategies, for the process measure. These are suggestions on different steps that may assist your team in accomplishing the aim you are focusing on. Interventions or change strategies are often grouped into “Guidelines/Protocols, Education, Electronic Medical Records Optimization, and Resources (inclusive of personnel and equipment)”.
As the local expert, you may have other ideas regarding how to best implement change in your hospital or ED. You should always feel free to reach out to your team leader and/or brainstorm these ideas with the other ED team leaders or participants working on similar aims in this collaborative.
WRITTEN POLICY/PROCEDURE
Change Strategies
- Written procedure/guideline should include vital sign norms for children (i.e., American Heart Association Pediatric Advanced Life Support (PALS), Pediatric Early Warning Score (PEWS), Emergency Severity Index (ESI)
- Conduct a pain assessment when appropriate
- Select a site-specific threshold for abnormal vitals
NOTIFICATION PROTOCOL
Change Strategies
- Establish criteria for activating the notification protocol
- Establish a protocol for addressing abnormal vital signs
- Key areas of focus: Which members of the care team should be contacted, Method of contact, Frequency of reassessments
- Establish a communication method to make the care team aware of abnormal vital signs
- Implement a visual alert system for high-risk patients
- Develop a recommended course of action when vital signs are out of range (e.g., initiate evidence-based guidelines, pathways, or protocols). Refer to the resource section for a list of evidence-based guidelines available through the EMSC Innovation & Improvement Center.
- Adopt a validated triage tool
- Implement standing physician orders in triage
EMR OPTIMIZATION
Change Strategies
- EMR alerts the care team when a vital sign is out of range
- Integrate a clinical decision support tool that evaluates a combination of factors (e.g., AAP’s Pediatric Septic Shock Collaborative’s Triage Identification Tool)
EDUCATION
Change Strategies
- Develop a training/educational program for the care team
- Learning objectives should include: Importance of vital signs and early recognition; What constitutes pediatric vital signs
- Identify training delivery modality (e.g., online, in-person staff meetings, peer to peer)
- Tabletop exercises
KNOWLEDGE REINFORCEMENT FOR CARE TEAM
Change Strategies
- Tabletop exercise to recognize patients with abnormal vital signs
- Posters in the triage area with normal vital ranges
- Posters with a scoring tool for abnormal vital signs
- Pocket cards/badge cards for the care team with normal vital ranges
- Direct feedback to the care team following chart audits
- Color-coded pages that correspond to the length-based tape
Below you will find suggested possible interventions, also called change strategies, for the process measure. These are suggestions on different steps that may assist your team in accomplishing the aim you are focusing on. Interventions or change strategies are often grouped into “Guidelines/Protocols, Education, Electronic Medical Records Optimization, and Resources (inclusive of personnel and equipment)”.
As the local expert, you may have other ideas regarding how to best implement change in your hospital or ED. You should always feel free to reach out to your team leader and/or brainstorm these ideas with the other ED team leaders or participants working on similar aims in this collaborative.
WRITTEN POLICY/PROCEDURE
Change Strategies
- Written procedure/guideline should include vital sign norms for children (i.e., American Heart Association Pediatric Advanced Life Support (PALS), Pediatric Early Warning Score (PEWS), Emergency Severity Index (ESI)
- Conduct a pain assessment when appropriate
- Select a site-specific threshold for abnormal vitals
NOTIFICATION PROTOCOL
Change Strategies
- Establish criteria for activating the notification protocol
- Establish a protocol for addressing abnormal vital signs
- Key areas of focus: Which members of the care team should be contacted, Method of contact, Frequency of reassessments
- Establish a communication method to make the care team aware of abnormal vital signs
- Implement a visual alert system to prompt reassessment of high-risk patients
- Develop a recommended course of action when vital signs are out of range (e.g., initiate evidence-based guidelines, pathways, or protocols). Refer to the resource section for a list of evidence-based guidelines available through the EMSC Innovation & Improvement Center.
- Adopt a validated triage tool
- Implement standing physician orders in triage
EMR OPTIMIZATION
Change Strategies
- “EMR alerts when a vital sign is out of range; examples include visual alerts on a track board, pop-up windows when charts are opened, and hard stops EMR alerts the care team when a vital sign is out of range
- Examples: visual alert system, pop-up windows, hard stops
- Develop an order set containing standard reassessment procedures
- Examples: frequency of vital sign assessments, dosing for common medications
- Integrate a clinical decision support tool that evaluates a combination of factors (e.g., AAP’s Pediatric Septic Shock Collaborative’s Triage Identification Tool)
EDUCATION
Change Strategies
- Develop a training/educational program for the care team
- Learning objectives should include: Importance of vital signs and early recognition; What constitutes pediatric vital signs
- Identify training delivery modality (e.g., online, in-person staff meetings, peer to peer)
- Tabletop exercises
KNOWLEDGE REINFORCEMENT FOR CARE TEAM
Change Strategies
- Tabletop exercise to recognize patients with abnormal vital signs
- Posters in the triage area with normal vital ranges
- Posters with a scoring tool for abnormal vital signs
- Pocket cards/badge cards for the care team with normal vital ranges
- Direct feedback to the care team following chart audits
- Color-coded pages that correspond to the length-based tape
Resources
- Abnormal Vital Signs - 2018 Cohort Intervention Bundle
Webpages
Emergency Severity Index (ESI): A Triage Tool for Emergency Department: Chapter 5. The Role of Vital Signs in ESI Triage | https://www.ahrq.gov/professionals/systems/hospital/esi/esi5.html
EMSC innovation & Improvement Center: Evidence Based Practice Repository for Guidelines
MDCalc online option to calculate PEWS: https://www.mdcalc.com/
Other Resources
American Heart Association. (2006). Pediatric Assessment. In M. Ralston, M. F. Hazinksi, A. L. Zaritsky, S. M. Schex-nayder & M. E. Kleinman (Eds.), Pediatric Advanced Life Support Provider Manual (pp. 9-16). Dallas, TX: American Heart Association.
Balamuth, F., Alpern, E. R., Grundmeier, R. W., Chilutti, M., Weiss, S. L., Fitzgerald, J. C., . . . Lautenbach, E. (2015). Comparison of Two Sepsis Recognition Methods in a Pediatric Emergency Department. Acad Emerg Med, 22(11), 1298-1306.
Bonafide, C. P., Brady, P. W., Keren, R., Conway, P. H., Marsolo, K., & Daymont, C. (2013). Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics, 131(4), e1150-1157.
Brent, A. J., Lakhanpaul, M., Thompson, M., Collier, J., Ray, S., Ninis, N., . . . MacFaul, R. (2011). Risk score to stratify children with suspected serious bacterial infection: observational cohort study. Arch Dis Child, 96(4), 361-367.
Craig, J. C., Williams, G. J., Jones, M., Codarini, M., Macaskill, P., Hayen, A., . . . McCaskill, M. (2010). The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ, 340, c1594.
Fleming, S., Thompson, M., Stevens, R., Heneghan, C., Pluddemann, A., Maconochie, I., . . . Mant, D. (2011). Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet, 377(9770), 1011-1018.
Gold, D. L., Mihalov, L. K., & Cohen, D. M. (2014). Evaluating the Pediatric Early Warning Score (PEWS) system for admitted patients in the pediatric emergency department. Acad Emerg Med, 21(11), 1249-1256.
Huang, D. T., Clermont, G., Dremsizov, T. T., & Angus, D. C. (2007). Implementation of early goal-directed therapy for severe sepsis and septic shock: A decision analysis. Crit Care Med, 35(9), 2090-2100.
Kulik, D. M., Uleryk, E. M., & Maguire, J. L. (2013). Does this child have bacterial meningitis? A systematic review of clinical prediction rules for children with suspected bacterial meningitis. J Emerg Med, 45(4), 508-519.
Nijman, R. G., Vergouwe, Y., Thompson, M., van Veen, M., van Meurs, A. H., van der Lei, J., . . . Oostenbrink, R. (2013). Clinical prediction model to aid emergency doctors managing febrile children at risk of serious bacterial infections: diagnostic study. BMJ, 346, f1706.
Nijman, R. G., Zwinkels, R. L., van Veen, M., Steyerberg, E. W., van der Lei, J., Moll, H. A., & Oostenbrink, R. (2011). Can urgency classification of the Manchester triage system predict serious bacterial infections in febrile children? Arch Dis Child, 96(8), 715-722.
O'Dempsey, T. J., Laurence, B. E., McArdle, T. F., Todd, J. E., Lamont, A. C., & Greenwood, B. M. (1993). The effect of temperature reduction on respiratory rate in febrile illnesses. Arch Dis Child, 68(4), 492-495.
Roland, D., Oliver, A., Edwards, E. D., Mason, B. W., & Powell, C. V. (2014). Use of paediatric early warning systems in Great Britain: has there been a change of practice in the last 7 years? Arch Dis Child, 99(1), 26-29.
Takahashi, T., Inoue, N., Shimizu, N., Terakawa, T., & Goldman, R. D. (2016). 'Down-triage' for children with abnormal vital signs: evaluation of a new triage practice at a paediatric emergency department in Japan. Emerg Med J, 33(8), 533-537.
Vaillancourt, S., Guttmann, A., Li, Q., Chan, I. Y., Vermeulen, M. J., & Schull, M. J. (2015). Repeated emergency department visits among children admitted with meningitis or septicemia: a population-based study. Ann Emerg Med, 65(6), 625-632 e623.
Van den Bruel, A., Aertgeerts, B., Bruyninckx, R., Aerts, M., & Buntinx, F. (2007). Signs and symptoms for diagnosis of serious infections in children: a prospective study in primary care. Br J Gen Pract, 57(540), 538-546.
Van den Bruel, A., Haj-Hassan, T., Thompson, M., Buntinx, F., & Mant, D. (2010). Diagnostic value of clinical features at presentation to identify serious infection in children in developed countries: a systematic review. Lancet, 375(9717), 834-845.
Verbakel, J. Y., MacFaul, R., Aertgeerts, B., Buntinx, F., & Thompson, M. (2014). Sepsis and meningitis in hospitalized children: performance of clinical signs and their prediction rules in a case-control study. Pediatr Emerg Care, 30(6), 373-380.
Verbakel, J. Y., Van den Bruel, A., Thompson, M., Stevens, R., Aertgeerts, B., Oostenbrink, R., . . . Buntinx, F. (2013). How well do clinical prediction rules perform in identifying serious infections in acutely ill children across an international network of ambulatory care datasets? BMC Med, 11, 10.
Watson, R. S., Carcillo, J. A., Linde-Zwirble, W. T., Clermont, G., Lidicker, J., & Angus, D. C. (2003). The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med, 167(5), 695-701.
Harriet Lane Handbook
Kirk, A. (2011). Pulmonology. In M. Tschudy & K. Acara (Eds.), The Harriet lane Hand-book. (19 ed., pp. 585). Philadelphia, PA: Elsevier Mosby.
Lennox, E. G. (2011). Cardiology. In M. Tschudy & K. Acara (Eds.), The Harriet Lane Hand-book (19 ed., pp. 170). Philadelphia, PA: Elsevier Mosby.
PAWS; PEWS
Monaghan, A. (2005). Detecting and managing deterioration in children. Paediatr Nurs, 17(1), 32-35.
Egdell, P., Finlay, L., & Pedley, D. K. (2008). The PAWS score: validation of an early warning scoring system for the initial assessment of children in the emergency department. Emerg Med J, 25(11), 745-749.
APLS Provider Manual
Ralston M, Hazinski MF, Zaritsky AL, Schex- nayder SM, Kleinman ME, eds. Pediatric assessment. In: Pediatric Advanced Life Support Provider Manual. Dallas, TX: American Heart Association; 2006:9–16
References
- Kazmierczak, Magdalena et al. “Outcomes of Patients Discharged from the Pediatric Emergency Department with Abnormal Vital Signs.” The American journal of emergency medicine. 57 (2022): 76–80.
- Weiss SL, Fitzgerald JC, Pappachan J, et al. Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med. 2015;191:1147-1157.
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med. 2013;14:686-693.
- Cruz, A. T. et al. Implementation of goal-directed therapy for children with suspected sepsis in the emergency department. Pediatrics 127, e758–e766 (2011).
- Morin, Luc et al. “The Current and Future State of Pediatric Sepsis Definitions: An International Survey.” Pediatrics / 149.6 (2022)
- Bourgeois, F. T. & Shannon, M. W. Emergency care for children in pediatric and general emergency departments. Pediatr. Emerg. Care 23, 94–102 (2007).
- Valentino, Katie et al. “Abnormal Vital Sign Recognition and Provider Notification in the Pediatric Emergency Department.” Journal of pediatric health care : official publication of National Association of Pediatric Nurse Associates & Practitioners. 34.6 (2020): 522–534.
- Sepanski, Robert J, Arno L Zaritsky, and Sandip A Godambe. “Identifying Children at High Risk for Infection-Related Decompensation Using a Predictive Emergency Department-Based Electronic Assessment Tool.” Diagnosis (Berl) 8.4 (2021): 458–468. Web.
- Balamuth, Fran et al. “Improving Recognition of Pediatric Severe Sepsis in the Emergency Department: Contributions of a Vital Sign-Based Electronic Alert and Bedside Clinician Identification.” Annals of emergency medicine : journal of the American College of Emergency Physicians. 70.6 (2017): 759–768.e2. Web.
- Eisenberg, Matthew A, and Fran Balamuth. “Pediatric Sepsis Screening in US Hospitals.” Pediatric research. 91.2 (2022): 351–358. Web.